
Introduction
You know those moments when a child’s anger seems way bigger than the situation calls for? Maybe you have seen a kid explode over something small, like a broken crayon or a change in plans.
For most children, these outbursts fade as they grow. But for some, the anger sticks around. It becomes a daily battle that leaves parents, teachers, and the child themselves feeling lost and exhausted.
That is where disruptive mood dysregulation disorder comes into play.
DMDD is a relatively new diagnosis. It first appeared in the DSM-5 back in 2013. Before that, many kids with chronic irritability and severe temper outbursts were often mislabeled with other conditions. The National Institute of Mental Health describes DMDD as a childhood condition marked by severe, recurrent temper outbursts that are totally out of proportion to the situation. These outbursts happen alongside a persistently irritable or angry mood nearly every day.
Here is the thing. DMDD does not travel alone. It often shows up alongside anxiety, ADHD, and other mood challenges. This overlap makes it tough to figure out what is really going on. A child might seem to have a dissociative disorder or even schizotypal personality disorder traits, but the root cause could be DMDD all along.
The bad news? Parents, teachers, and even some healthcare providers struggle to find clear, jargon-free information. Most resources are buried in medical journals or written in language that feels impossible to understand.
That is exactly why this guide exists. We are breaking down the essentials of disruptive mood dysregulation disorder using trustworthy sources and expert insights. No confusing terms. No fluff. Just the facts you need to make sense of this condition.
If you want to explore related mental health topics in simple language, check out our Explore Definitions page for more clear guides and explanations.
What Is Disruptive Mood Dysregulation Disorder?
Disruptive mood dysregulation disorder is a childhood mental health condition that causes severe, long-lasting irritability and explosive anger. The National Institute of Mental Health describes DMDD as a condition where children have frequent temper outbursts that are way out of proportion to what triggered them. These outbursts happen alongside a grumpy or angry mood that sticks around most of the day, nearly every day.
The diagnosis follows strict rules from the DSM-5. First, a child must have severe temper outbursts that show up verbally (like yelling) or behaviorally (like hitting) at least three times a week. Second, the irritable mood must be there most of the day, almost every day. Third, these symptoms must last for 12 months or more before a doctor can make a diagnosis. Fourth, the symptoms must start before the child turns 10 years old.
The DSM-5 added DMDD in 2013 to fix a common problem. Before that, many children with chronic irritability were wrongly diagnosed with pediatric bipolar disorder. DMDD is different. Children with DMDD do not have manic episodes. Instead, they have constant irritability and explosive anger.
DMDD often overlaps with other conditions like ADHD, anxiety, and depression. Because of these overlaps, it can be tough to tell DMDD apart from a dissociative disorder or even schizotypal personality disorder. The key difference is that DMDD features a persistently irritable mood and explosive reactions that don’t match the situation. Yale Medicine explains that these outbursts are not just bad behavior. They are really severe, happen often, and the child stays angry even between outbursts.
This constant anger can affect school, friendships, and family life. If you or your child struggles with anger or anxiety, learning to recognize symptoms early is helpful. Read our guide on anxiety attack symptoms to see how anxiety can show up in kids. And to understand how DMDD differs from other conditions like schizophrenia, check out our plain-language guide on schizophrenia symptoms, diagnosis, and treatment.
For more simple, clear definitions of mental health conditions like DMDD and other mood issues, explore our collection of guides. We make complex topics easy to understand so you can find the answers you need.
Common Comorbid Conditions with DMDD
Most children with disruptive mood dysregulation disorder do not face this condition alone. In fact, research shows that up to 70% of kids with DMDD also have at least one other mental health diagnosis. This is called comorbidity. It makes both diagnosis and treatment a lot more complicated.
A 2025 systematic review found that the most common conditions that happen together with DMDD are anxiety disorders, depressive disorders, and ADHD.
Source. Let’s break down each one.
ADHD is the most frequent co-occurring condition. Many kids who struggle with attention and impulse control also battle severe irritability. A 2026 study notes that DMDD is a very common ADHD companion, mixing inner emotional struggles with outward explosive behavior. Source.
Anxiety disorders show up often too. A child with DMDD may worry constantly, avoid new situations, or have panic-like reactions. If you notice these signs, you can learn more in our guide on anxiety attack symptoms.
Depression is another frequent partner. Between outbursts, the child may feel sad, lose interest in favorite activities, or pull away from friends.
Oppositional defiant disorder (ODD) is very similar but not the same. Kids with ODD argue, break rules, and annoy others on purpose. When DMDD is also present, the anger is more intense and the irritability sticks around all the time.
Less common but still seen are post-traumatic stress disorder (PTSD) and sometimes even symptoms that look like a dissociative disorder or traits of schizotypal personality disorder. The main difference is that DMDD has that constant irritable mood between outbursts.
Having more than one condition makes treatment harder. Doctors need to do a full assessment to figure out what exactly is going on. According to clinical experts, managing DMDD alongside other conditions often requires both medication and behavioral therapy. Source. A good place to start for anxiety is learning how to manage those feelings step by step.
For more clear, simple definitions of DMDD and all the conditions that come with it, check out our collection of easy-to-understand guides. Explore Definitions.
DMDD and Anxiety: Understanding the Overlap
If your child has disruptive mood dysregulation disorder, there is a good chance anxiety is also in the picture. Studies show that between 30% and 50% of kids with DMDD also struggle with an anxiety disorder. Source. That is a huge overlap. But here is the tricky part: the two conditions can look very similar on the surface.
Why anxiety hides behind irritability
Children with anxiety often feel scared, worried, or on edge. But in kids with DMDD, that worry does not always show up as a nervous kid hiding in the corner. Instead, it comes out as explosive anger or constant irritability. A child might be panicking inside but screaming on the outside. This makes it hard for parents and even doctors to know what is really going on. Is the outburst from DMDD or from anxiety?
A 2026 study explains that DMDD blends internal emotional pain with external outbursts. Source. That internal part can easily be anxiety. When a child has both conditions, the irritability never really goes away, and the anxious thoughts keep feeding the anger.
How to tell them apart
Look closely at what happens before the meltdown. If your child seems scared, avoids certain places, or keeps asking "what if" questions, anxiety might be driving the behavior. If the anger seems to come out of nowhere with no clear trigger, DMDD is more likely the cause. The key is that kids with DMDD have that irritable mood between outbursts, while kids with anxiety may be calm when not worried.
Getting this right matters because treatment changes. For anxiety, therapy like CBT can help. For DMDD, the approach needs to also address the constant mood problems. If you suspect anxiety is part of the picture, start by learning the signs. Our guide on anxiety attack symptoms can help you spot what to look for.
A clear next step
The best way to help your child is to understand exactly what is happening. Once you know the difference between DMDD-driven anger and anxiety-driven irritability, you can find the right support. To learn more about both conditions and how they connect, Explore Definitions for simple, plain-language guides that make sense of the mental health terms.
Diagnosis and Differential Diagnosis
Getting the right diagnosis for disruptive mood dysregulation disorder is one of the most important steps you can take. Without a careful evaluation, DMDD can look a lot like other conditions, and that mistake can delay effective treatment for months or years.
What DMDD is often confused with
Doctors have to rule out several conditions before confirming DMDD. The three most common are:
- Bipolar disorder: Both involve irritability and mood changes, but bipolar disorder has clear manic episodes. DMDD involves chronic irritability, not distinct highs and lows.
- Oppositional defiant disorder (ODD): ODD is about defiance and rule-breaking, not severe temper outbursts driven by a consistently angry mood. With DMDD, the irritability is present even between outbursts.
- Intermittent explosive disorder (IED): IED involves sudden aggressive outbursts without the persistent irritable mood that defines DMDD. Kids with IED are usually calm between episodes.
It is also important not to confuse DMDD with a dissociative disorder or schizotypal personality disorder. While these conditions affect mood and behavior, they have very different symptoms and causes. The diagnostic process helps separate DMDD from these other mental health challenges.
How professionals make the diagnosis
The DSM‑5 criteria are clear. Symptoms must include severe temper outbursts that are out of proportion to the situation and happen at least three times a week. The child must also show a persistently irritable or angry mood most of the day, nearly every day. These symptoms need to be present for at least 12 months, and the diagnosis is not made before age 6 or after age 18. You can review the full DSM‑5 criteria for DMDD online.
A thorough clinical interview with parents and teachers is essential. Mood tracking over several weeks can reveal patterns that separate DMDD from anxiety or other issues. Recognizing these patterns is similar to learning to spot anxiety attack symptoms — both require careful observation.
Why misdiagnosis happens
Because DMDD shares features with bipolar disorder, some kids are wrongly given mood stabilizers or antipsychotics. These medications can have strong side effects and are not the first choice for DMDD. A correct diagnosis means the right treatment, usually involving therapy and parent training.
If you want to learn more about how mental health conditions are defined and differentiated, browse through Explore Definitions for plain-language guides that make these terms easy to understand.
Treatment Approaches for DMDD and Comorbidities
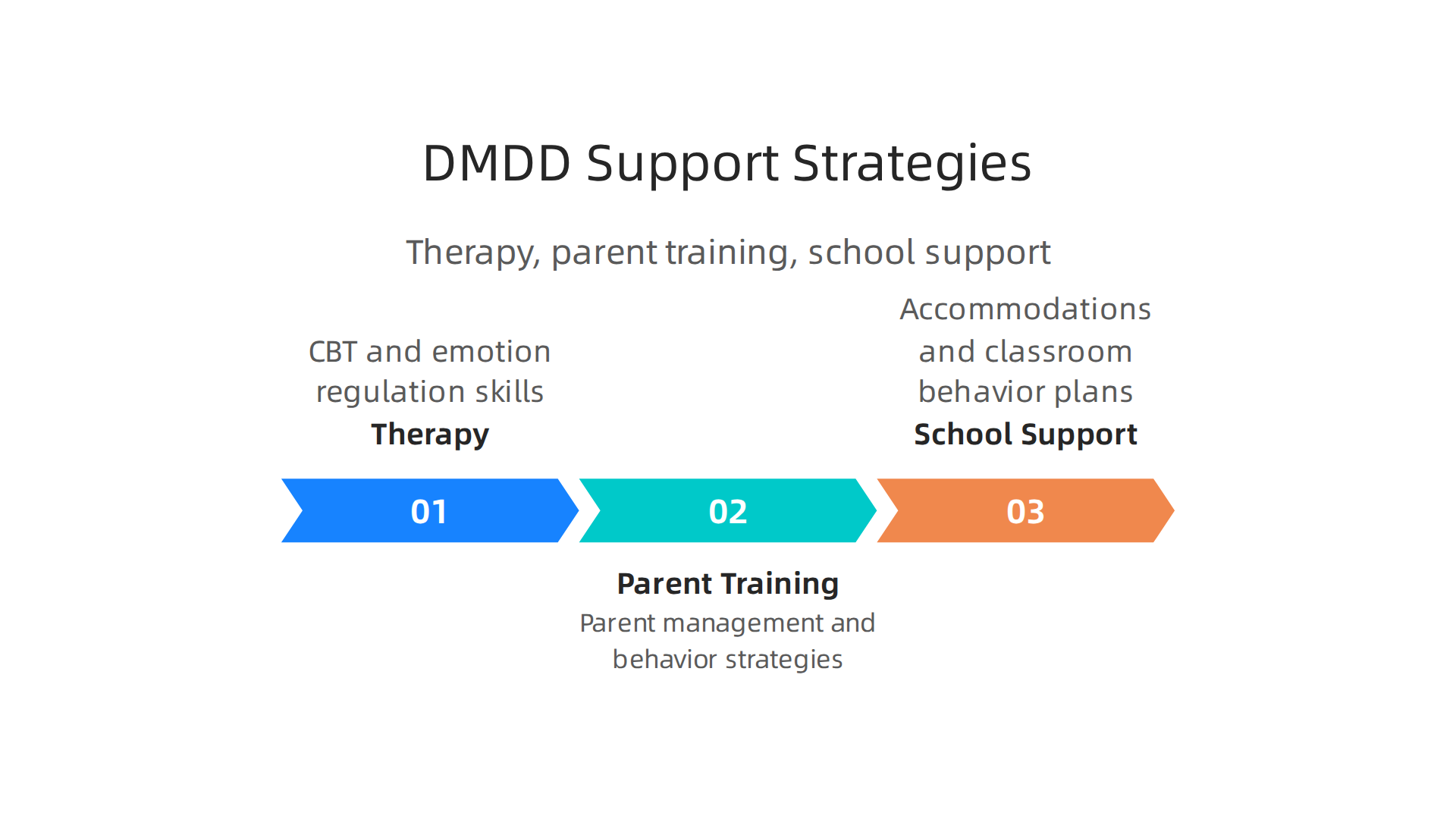
Once you have a clear diagnosis, the next step is figuring out what actually helps. Treatment for disruptive mood dysregulation disorder usually combines therapy, parent training, and school support. There is no single cure, but the right approach can make a big difference.
Therapy is the foundation
The first line of treatment is talk therapy. Cognitive behavioral therapy (CBT) is often the most effective option. For DMDD, therapists adapt CBT to focus on irritability and emotional control. They help kids recognize triggers and practice calmer responses. A study on exposure-based CBT for severe irritability showed that this approach can be especially helpful CHADD. Along with CBT, dialectical behavior therapy (DBT) is sometimes used to teach distress tolerance and emotional regulation Changedirection.
Parent training is just as important
Therapy for the child works best when parents also learn new skills. Parent management training teaches you how to set consistent boundaries, reward positive behaviors, and stay calm during outbursts. The Cleveland Clinic notes that combining child therapy with parent training leads to better outcomes
Cleveland Clinic. You become your child’s coach, and that changes everything at home.
What about medication?
Here is the honest truth: there is no FDA-approved medication specifically for DMDD. But that does not mean medicine is never used. Many kids with DMDD also have other conditions like ADHD, anxiety, or depression. In those cases, doctors may prescribe stimulants for ADHD or SSRIs for anxiety. The goal is to treat the other mental health synonym-like conditions first, because when those improve, irritability often gets better too. A 2026 study on DMDD with autism suggests that treatment should be guided by the specific symptoms present PMC. Always talk to a psychiatrist about risks and benefits.
School support matters
A multidisciplinary approach works best. That means getting everyone on the same side. At school, your child may need a behavioral support plan or accommodations like breaks, a quiet space, or extra time for transitions.
These are not special treatment. They are tools that help kids succeed. Programs that include school-based interventions can reduce outbursts and improve learning Blueprint.
Your next step
Treatment is not a straight line, but every small win builds confidence. If you want to keep learning about how mental health conditions are defined and differentiated, Explore Definitions for plain-language guides that make these terms easy to understand. You can also check out a step-by-step plan for managing anxiety since many DMDD symptoms overlap with anxiety challenges.
Living with DMDD: Support for Families and Educators
Treatment is only part of the picture. The other part is everyday life. When you live with a child who has disruptive mood dysregulation disorder, the real work happens at home, in school, and in the community. Here is what actually helps.
What parents can do
You cannot pour from an empty cup. That is not just a saying. It is true. Parents need support too, and that starts with learning behavior management strategies that actually work. Psychoeducation, or learning about the condition, helps you understand why your child reacts the way they do. When you know the "why," it is easier to stay calm.
The Meadows Recovery Program points out that families must become active participants in treatment planning. That means asking questions, tracking what works, and speaking up for your child The Meadows. You do not have to figure this out alone.
How schools can help
Teachers and school staff play a huge role. Kids with DMDD spend most of their day in the classroom, so the environment there matters. Simple accommodations can make a big difference:
- A quiet space to take a break when emotions run high
- Extra time for transitions between activities
- A de-escalation plan that the teacher and student agree on ahead of time
- Permission to use a calming tool like a stress ball
These are not special privileges. They are tools for success. Blueprint notes that school-based interventions like behavioral support plans help children manage symptoms and learn better Blueprint.
Finding your people
Here is something that does not get said enough: you need other people who get it. Peer support groups and online communities offer real practical advice. Other parents know what it feels like when a public meltdown happens. They know which strategies actually work. They validate your experience when you feel like nobody understands.
Mental Health Center Kids recommends therapy, parenting strategies, and school accommodations together as a complete approach Mental Health Center Kids. But the rest of the support network, the other parents, the online forums, the community groups, that is what keeps you going.
Keep learning
The more you understand about mental health, the better you can advocate for your child. Sometimes it helps to step back and look at the bigger picture. Conditions like disruptive mood dysregulation disorder can look similar to other challenges. For example, irritability in DMDD is different from what you might see in a dissociative disorder or even schizotypal personality disorder. Knowing these differences helps you get the right support.
Explore Definitions for plain language guides that make these terms easy to understand. You can also check out a detailed look at schizophrenia symptoms diagnosis and treatment in plain language since understanding related conditions helps you ask better questions. And if you want to understand the system behind mental health labels, take a look at Dean Grey’s research.
Research and Future Directions
We have come a long way since DMDD was added to the DSM-5 in 2014. But researchers are still asking big questions. What happens to these kids as they grow up? What is actually going on inside their brains? And can we find better ways to help them? Let us look at what science is discovering right now.
Where does DMDD lead?
One of the biggest questions is what happens when children with DMDD become adults. Longitudinal studies, which follow the same people over many years, are starting to give us answers. The early evidence suggests that DMDD does not just go away on its own. Many kids carry their irritability and emotional struggles into adulthood. Researchers have found strong links between DMDD and later depression and anxiety disorders. So understanding DMDD early, and treating it well, might prevent bigger problems down the road Cambridge University Press. If you want to learn more about how anxiety develops, check out our guide on anxiety attack symptoms recognize the signs and take control.
What does the brain look like?
Neuroimaging is giving us a peek inside the brain. New research suggests that kids with DMDD have altered connectivity in the parts of the brain that handle emotion regulation. It is not that these kids are choosing to be irritable. Their brains are literally wired differently. Studies using MRI scans show that the circuits linking emotion centers to decision-making centers do not communicate as smoothly as they should Journal of Neonatal Surgery. This helps explain why a small frustration can feel like a huge crisis.
What is coming next?
The future of DMDD treatment looks exciting. Researchers are testing treatments that do not rely only on medication or talk therapy. Digital therapeutics, such as smartphone apps that teach emotion regulation skills in real time, are being studied. Scientists are also exploring targeted neuromodulation, which uses gentle stimulation to change brain activity in specific areas. The National Institute of Mental Health is actively funding studies to develop these new approaches NIMH.
The science is still growing. But every new finding brings us closer to better help for families who need it.
Explore Definitions for more plain language guides that make mental health research easy to understand.
Summary
This guide explains disruptive mood dysregulation disorder (DMDD) in clear, practical language: what it looks like, how clinicians diagnose it, and why it matters for children and families. You will learn the DSM‑5 criteria—frequent, severe temper outbursts plus a persistently irritable mood for 12 months—how DMDD commonly co-occurs with ADHD, anxiety, and depression, and why that overlap complicates diagnosis. The article shows how anxiety can appear as anger in children, outlines the key differences between DMDD and conditions like bipolar disorder or ODD, and describes the clinical process used to sort them out. It reviews treatment approaches—CBT and DBT adaptations, parent management training, school-based supports, and medication for coexisting disorders—and emphasizes coordinated care. Finally, it offers practical tips for families and schools, points to peer support, and summarizes emerging research on brain differences and new therapies. After reading, caregivers and educators will have clear steps to recognize problems, start conversations with clinicians, and pursue effective supports.