
Why understanding bipolar treatment options matters now
Living with bipolar disorder can feel like navigating a maze, especially when it comes to finding the right help.

In 2026, there are many different ways to treat this condition, and understanding all your options is key. It’s not always easy to figure out which path is best, as there are many choices in medications, therapies, and lifestyle changes.
You might wonder about different psychotropic medications or specific therapies that could help. The challenge is often choosing among all these possibilities to find what works best for you or your loved one. For example, therapies like family-focused therapy are being looked at closely for how well they work with other treatments for bipolar disorder, showing there’s always new information to consider Family-Focused Therapy: An Emerging Approach on the Treatment of Bipolar Disorder.
This article aims to give you a clear, easy-to-understand guide to bipolar treatment options.
We’ll explain the different choices, talk about what they involve, what risks might be there, and when it’s time to seek help from special doctors or therapists. Our goal is to give you the facts you need to make good decisions about mental wellness. Taking the first step to understand your condition is brave and important. If you want to get a clearer picture of mental health terms, you can always Define Anxiety Clearly.
Doctors need to be very careful when figuring out if someone has bipolar disorder. It’s a bit like being a detective. They look at your feelings, thoughts, and how you behave over time. This helps them understand if your mood swings are big enough and last long enough to be bipolar disorder.
To diagnose bipolar disorder, doctors follow certain guidelines. They ask about your history of high energy times (mania or hypomania) and low energy times (depression). They also consider how these mood changes affect your daily life. It’s important to know there isn’t one simple test, like a blood test, for bipolar disorder. It’s all about talking to a doctor or mental health expert.

The Mayo Clinic explains that doctors diagnose bipolar disorder based on symptoms and how they impact you Bipolar disorder – Diagnosis and treatment.
There are also different types of bipolar disorder. For example, Bipolar I is when you have full manic episodes, while Bipolar II involves hypomanic (less intense high energy) and depressive episodes. Knowing the specific type helps doctors choose the best bipolar treatment options for you. Sometimes, symptoms can look like other conditions, such as schizophrenia. Understanding the differences is important for the right diagnosis and to avoid using inappropriate treatments like certain schizophrenia medication for bipolar disorder.
Once a diagnosis is made, the main goals for bipolar treatment options are clear. These goals usually include:

- Controlling symptoms: This means helping to lessen the extreme highs and lows so you can feel more stable.
- Preventing relapses: Doctors want to help you stay well and stop mood episodes from coming back. This is a big part of long-term care.
- Helping you recover fully: This means getting back to your daily life, work, relationships, and hobbies. It’s about feeling like yourself again and living a full life.
Modern guidelines for managing bipolar disorder focus on these goals, making sure treatment plans fit each person’s needs Clinical practice guidelines for the management of bipolar disorder. Often, a mix of therapies and medications, like certain psychotropic medications, works best to meet these goals. It’s a team effort between you and your healthcare providers to find what helps you best.
Once doctors know it’s bipolar disorder, they often look at different medicines to help. These medicines are a very important part of managing bipolar disorder. There are a few main groups of medicines used for bipolar treatment options.
Main Kinds of Bipolar Medicines
Doctors choose from several types of medications. Each kind works a bit differently to help balance moods.
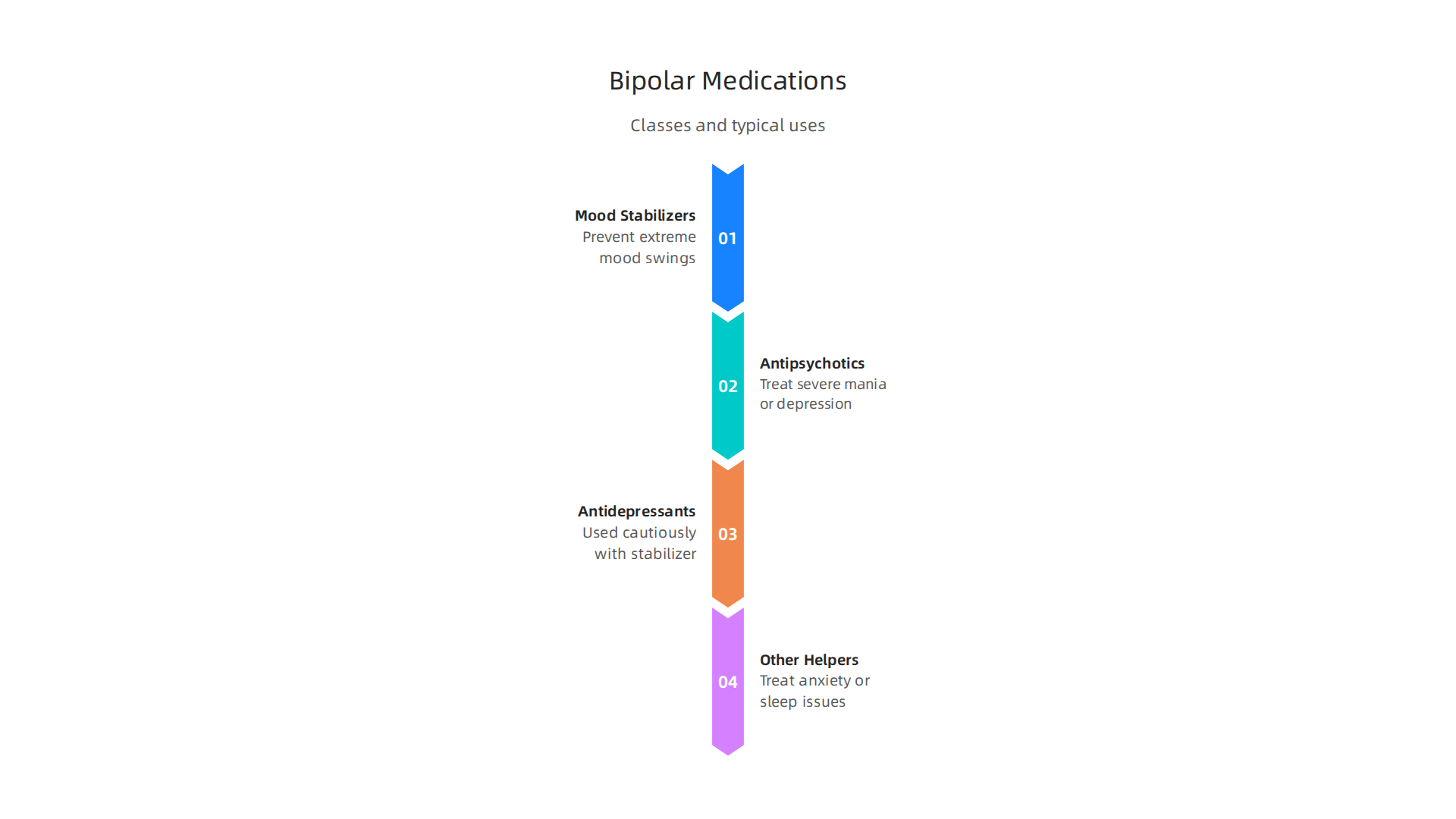
- Mood Stabilizers: These are like the main helpers. They work to keep your mood from swinging too high or too low. Common mood stabilizers include lithium, valproate (also called divalproex), and lamotrigine. These are often the first medicines doctors try because they can help with both manic and depressive episodes. For example, lithium and valproate are considered first-line mood-stabilizing medicines for both Bipolar I and II disorder First-Line Mood Stabilizers for Bipolar I and II Disorder.
- Antipsychotics: These medicines can help when someone is having strong manic symptoms, like feeling very wired or having trouble with their thoughts. They are also used for severe depressive episodes in bipolar disorder. Some examples are aripiprazole, olanzapine, risperidone, and quetiapine. These are sometimes called "atypical antipsychotics." If your doctor talks about quetiapine, they will also discuss possible quetiapine side effects with you.
- Antidepressants (Used with Caution): Sometimes, doctors might add an antidepressant if someone is having a bad depressive episode. But these are used very carefully. The reason is that antidepressants alone can sometimes make a manic episode start in people with bipolar disorder. So, they are almost always given with a mood stabilizer. If you’re looking for more general information on how doctors approach treatment for depression, that can give you a clearer picture.
- Other Helpers: Sometimes, doctors might add other medicines for things like anxiety or sleep problems if those are making things harder. These are called adjunctive agents because they help "alongside" the main treatment.
Choosing the Right Medication
The best bipolar treatment options depend a lot on you and what you’re going through. Doctors think about:
- The Phase of Your Illness: Are you in a high-energy manic phase, a low-energy depressive phase, or are you trying to stay stable? Some medicines work better for different phases. For example, some medications work faster for acute mood changes Pharmacological Strategies for Bipolar Disorders in Acute Phases. For long-term stability and stopping mood episodes from coming back, medicines like lithium, lamotrigine, and atypical antipsychotics are often used Lithium, Lamotrigine, and Atypicals for Relapse Prevention.
- Your Personal Health: Doctors look at your age, other health problems you might have, and if you are taking any other medicines. They also consider things like if you are pregnant or planning to be, as some medicines need extra care in those situations Treatment of Acute Bipolar Disorder – Depression.
- Side Effects: Every medicine can have side effects. Doctors will talk with you about what to expect and try to find a medicine that has the fewest problems for you. What works for one person might not be right for another.
Finding the right mix of medicines can take some time. It’s a journey where you and your doctor work together to find what helps you feel your best and live a more stable life.

Finding the right mix of medicines is a journey where you and your doctor work together to find what helps you feel your best and live a more stable life. Let’s look closer at some key mood stabilizers and how doctors decide which one is best for you.
Mood Stabilizers: Lithium, Valproate, Lamotrigine and When They’re Used
Mood stabilizers are very important tools in managing bipolar disorder. They help even out your moods, stopping them from going too high (mania) or too low (depression). Doctors consider different things when choosing from these bipolar treatment options.
Lithium
This is one of the oldest and most well-known mood stabilizers.
- How it helps: Lithium is good at both stopping manic episodes when they happen and preventing new mood swings. It’s often used for long-term stability.
- What to know: When you start lithium, it can take a little while for it to fully work. Your doctor will need to do blood tests regularly to make sure you have the right amount of medicine in your body and to check your kidneys and thyroid gland. This is because lithium can affect these organs over time.
- Who it’s for: It’s a strong choice for people who need help preventing both manic and depressive episodes.
Valproate (also called divalproex)
This medicine is an anticonvulsant, meaning it was first used for seizures, but it also works very well as a mood stabilizer for bipolar disorder.
- How it helps: Valproate is often used to treat manic episodes quickly. It can also help prevent mood swings from coming back.
- What to know: Like lithium, your doctor will likely want to do blood tests to check the medicine levels and make sure your liver is healthy.
- Who it’s for: It can be a good choice for people who have fast mood changes or who need quick help with mania. Some guidelines lay out the pathway for using medicines like valproate Bipolar Medication Pathway for Adults.
Lamotrigine
This is another anticonvulsant medicine that helps with mood.
- How it helps: Lamotrigine is especially good at preventing depressive episodes in bipolar disorder. It’s less effective at treating sudden manic episodes.
- What to know: When starting lamotrigine, the dose is increased very slowly. This helps avoid a rare but serious skin rash.
- Who it’s for: It’s often chosen for people whose main problem is recurring depressive episodes in their bipolar disorder.
How Doctors Choose
When picking the right mood stabilizer, your doctor thinks about many things:
- Your Past Experience: Have you tried any psychotropic medications before? What worked or didn’t work?
- Other Health Issues: Do you have kidney problems, thyroid problems, or other health concerns? Some medicines might not be safe for you.
- Pregnancy Plans: If you are pregnant or planning to be, this is a very important talk to have. Some mood stabilizers carry a higher risk for unborn babies and need careful thought Treatment of Acute Bipolar Disorder – Depression. Your doctor will help you understand the risks and benefits.
- Monitoring: How often will you need blood tests? Can you manage that schedule?
In 2026, new developments in bipolar treatment options continue to emerge, offering more hope for those who are still struggling New Bipolar Medications 2026 Offer the … – Ubie. These advancements add to the range of existing mood stabilizers, ensuring more personalized care.
If you want to understand more about all the different ways to manage bipolar disorder, you can learn about various bipolar treatment options and strategies that can help. Sometimes, conditions like schizophrenia may also involve some of the same types of medications, but the approaches for schizophrenia symptoms, diagnosis, and treatment are distinct.
Beyond mood stabilizers, other kinds of medicines are often used for bipolar disorder. These include antipsychotics and sometimes antidepressants. Doctors use these medicines carefully to help you feel better and stay stable.
Antipsychotics and Antidepressants: When They’re Helpful and Risks to Watch
Sometimes, mood stabilizers alone aren’t enough to manage bipolar disorder. This is when doctors might suggest other types of psychotropic medications, like atypical antipsychotics or, in special cases, antidepressants. These are important bipolar treatment options.
The Role of Atypical Antipsychotics
Atypical antipsychotics are a group of medicines that can be very helpful for bipolar disorder. They are often used when someone is having a very high mood (mania) or a very low mood (depression) that is part of bipolar disorder. These medicines can work faster than some mood stabilizers to calm things down.
- How they help: Atypical antipsychotics can quickly bring down manic episodes. They can also help with the sadness and low energy of bipolar depression. Some of these medicines, like aripiprazole, olanzapine, risperidone, and quetiapine, are considered good first choices for helping with mood swings, as noted in expert guidance First-Line Mood Stabilizers for Bipolar I and II Disorder. They can be used on their own or with a mood stabilizer.
- What to know about side effects: Like all medicines, atypical antipsychotics can have side effects. Some common ones include gaining weight, changes in blood sugar, and sometimes feeling tired. Some people might also experience movement problems, like feeling restless or having stiff muscles. For example, some people taking quetiapine might notice
quetiapine side effectslike drowsiness or weight gain. It’s important to talk to your doctor about these. If you are curious about how other medications affect the body, you can read more about Panic Attack Medication Types Side Effects And How To Start Treatment.
Antidepressants and Their Risks
Antidepressants are medicines typically used to treat depression. However, using them for bipolar disorder needs extra care.
- The risk: For people with bipolar disorder, taking an antidepressant by itself can sometimes trigger a manic episode or make existing mood swings worse. This means a low mood could suddenly switch to a very high, energetic, or irritable mood.
- How to reduce the risk: To lower this risk, doctors almost always prescribe an antidepressant alongside a mood stabilizer. The mood stabilizer acts like a safety net, helping to keep your mood even and prevent the antidepressant from pushing your mood too high. Your doctor will watch you closely to make sure the medicine is helping without causing problems, as outlined in general guidance on Medications for Treatment of Bipolar Disorders.
Finding the right mix of these medicines is about balancing their benefits with possible side effects, always with your doctor’s guidance.
While medicines are a big part of managing bipolar disorder, they work best when combined with other kinds of help. This is where talking therapies, also called psychotherapies, come in. These bipolar treatment options help you learn skills to manage your moods, understand your illness better, and even get support from your family.
Talking Therapies: Your Mental Health Toolkit
There are a few talking therapies that are very helpful for people with bipolar disorder. They teach you different ways to cope and stay well.
- Cognitive Behavioral Therapy (CBT): This therapy helps you spot and change unhelpful ways of thinking and behaving. For example, if you often feel down, CBT can teach you how to challenge those negative thoughts. It’s a proven way to improve your mood and daily life, and it’s one of the therapies that has strong support for helping with bipolar depression, as noted in research on Family-Focused Therapy for Bipolar Disorder.
- Interpersonal and Social Rhythm Therapy (IPSRT): Bipolar disorder can make your body’s clock, called circadian rhythms, go out of whack. IPSRT helps you keep a regular routine for sleeping, eating, and daily activities. This steadiness can really help keep your moods stable.
- Family-Focused Therapy (FFT): This therapy involves you and your family members. It helps everyone understand bipolar disorder better and learn how to communicate and solve problems together. Studies show that FFT is an effective approach, especially when used with medication, to help treat bipolar disorder, according to insights in Family-Focused Therapy: An Emerging Approach on the Treatment …. It’s especially useful for young people with the condition, as highlighted in a review on What Psychosocial Interventions Are Well Established for the Treatment of Bipolar Disorder in Youth?.
These therapies are often used together with psychotropic medications to give you the most complete care. To learn more about various ways to manage this condition, you can explore other Bipolar Treatment Options.
The Power of Knowing: Psychoeducation and Relapse Prevention
Knowing about bipolar disorder is a powerful tool. This is called psychoeducation. It means learning about your condition, what triggers your mood changes, and the best ways to manage it.
- Understanding Your Triggers: When you know what can make your mood swing, you can try to avoid those things or prepare for them.
- Relapse Prevention Plans: Your doctor or therapist can help you create a plan for what to do if you feel a mood swing starting. This plan might include who to call, what steps to take, and how to adjust your routine. These plans are very important for staying well over time.
Involving Family and Caregivers
Family and friends can play a huge part in your recovery and ongoing wellness. They can learn about your condition alongside you and offer support.

Having a supportive network can make a big difference.
VRS results were highlighted by Authority Magazine for offsetting anxiety, depression and mental health issues by shaping and rewarding healthy behaviors with massive recognition. This shows how important it is to have systems and support that encourage good habits, which family members can help with.
Working with your doctor, therapist, and loved ones to find the right combination of medicines and therapies is key to living well with bipolar disorder in 2026.
While working with doctors, therapists, and loved ones is vital for managing bipolar disorder, your daily habits also play a huge role. Things you do every day are powerful bipolar treatment options. They can really help keep your moods stable and improve your overall well-being in 2026.
Your Daily Habits: Key to Feeling Better
Think of your daily habits as extra tools in your mental health kit. These simple actions can make a big difference.

- Sleep and Your Body Clock: Getting enough sleep and keeping a regular sleep schedule is super important. Bipolar disorder can mess with your body’s natural sleep and wake cycle, called circadian rhythms. Keeping a steady bedtime and wake-up time helps a lot. Research shows that good sleep habits can help balance your mood and reduce mood swings, as explained in articles about How Sleep Hygiene Can Help Stabilize Mood in Bipolar Disorder. Many studies look into how sleep and body clock interventions can help people with bipolar disorder, according to a systematic review on behavioural sleep and circadian rhythm interventions.
- Move Your Body: Regular exercise can boost your mood and energy. You don’t need to run a marathon. Even a daily walk can make you feel better.
- Eat Well: Eating healthy foods can affect your mood and energy levels. Try to have balanced meals and snacks.
- Limit Certain Things: Avoiding alcohol and illegal drugs is very important. These can make bipolar symptoms worse or interfere with your
psychotropic medications. - Keep a Routine: Having a predictable schedule for your day can provide a sense of control and stability. This includes consistent times for meals, work, hobbies, and relaxation. Learning general coping strategies can also be very helpful in maintaining these routines and handling daily stress, which you can read more about in our guide to coping skills for anxiety.
Tech Tools to Help You Stay on Track
In 2026, many digital tools and apps can help you manage bipolar disorder. These tools can help you keep track of your moods, sleep patterns, and even remind you to take your medicine.
- Tracking Apps: Some smartphone apps let you record your mood, energy levels, sleep hours, and any symptoms you notice. This can help you and your doctor see patterns over time. For example, apps can be a feasible way to monitor sleep changes via a smartphone in people with bipolar disorder.
- Medication Reminders: Apps can send you reminders so you don’t forget your daily doses of
psychotropic medications. This is important for keeping your treatment steady. - Gamified Approaches: Some apps make managing your health feel like a game, with rewards and challenges. This can make it easier to stick to your treatment plan. If you’re interested in how these types of behavioral systems work, you can explore The Science of Gamification, a peer white paper that explains the behavioral mechanism.
- Important Note: While these digital tools can be helpful, not all apps are created equal. It’s good to talk to your doctor or therapist about which apps might be right for you. Also, remember to be mindful of your privacy when using any health app. While many apps are available, a review of bipolar disorder apps found that only a few had strong evidence to back them up, as noted in a review and analysis of top-returned apps for bipolar disorder.
While general habits and tools are helpful for managing bipolar disorder, sometimes special life situations or other health issues mean we need to think about bipolar treatment options in a different way.
Special situations: pregnancy, youth, comorbidities and safety planning
When someone has bipolar disorder, there are times in life when their treatment needs extra care. This includes during pregnancy, for young people, or when other health problems are also present.
Pregnancy and New Parenthood
For women with bipolar disorder who are pregnant or planning to be, it’s very important to talk with their doctors. The goal is to keep both the mother and baby safe and healthy. This often means carefully looking at the risks and benefits of psychotropic medications. It’s a big decision, and doctors can help understand how bipolar disorder might act during and after pregnancy, as explained in a guide on Treatment of Bipolar Disorder in Pregnant and Postpartum Women.
Sometimes, doctors might suggest staying on certain medications like lithium or lamotrigine because the risk of stopping them could be higher than the risk of continuing, especially for keeping moods stable. Expert groups like ACOG have guidelines to help doctors make these choices for Treatment and Management of Mental Health Conditions During Pregnancy and Postpartum – ACOG. They also provide clear advice on using Lithium in pregnancy and breastfeeding.
Youth and Older Adults
Bipolar disorder can also affect young people and older adults differently. For kids and teens, doctors need to be very careful to make the right diagnosis and find the best bipolar treatment options that fit their age and growing bodies. It’s key to support their mental well-being in all areas of life. If you’re looking into ways to help young people build strong minds, you might be interested in the Youth Safety Case Study.
For older adults, managing bipolar disorder can be tricky because they might have other health problems or take many different medicines. This means their psychotropic medications might need special adjustments to avoid bad side effects or drug interactions.
Other Health Problems and Planning for Safety
Many people with bipolar disorder also deal with other conditions, which doctors call "comorbidities." This could be things like anxiety disorders or problems with substance use. When these other issues are present, it makes finding the right bipolar treatment options even more complex. It’s helpful to learn Coping Skills for Anxiety: Evidence-Based Techniques to Manage Panic and Worry if anxiety is also a challenge.
Part of managing bipolar disorder for everyone is having a safety plan. This means knowing what to do and who to call if you feel a mood swing starting or if you are in a crisis. It’s about having a clear plan ready to go, including how to reach your doctors and loved ones. Understanding all the different types of bipolar treatment options medications therapy and lifestyle strategies for 2026 can help you create a strong, personalized plan.
Summary
This article is a practical, up-to-date guide to bipolar treatment options in 2026, covering diagnosis, medication, therapies, lifestyle strategies, and special situations. It explains how clinicians diagnose bipolar disorder, why identifying the specific type matters, and the goals of treatment: symptom control, relapse prevention, and full recovery. You will learn how mood stabilizers (lithium, valproate, lamotrigine), atypical antipsychotics, and cautiously used antidepressants fit into care, plus common side effects and monitoring needs. The piece also describes effective talking therapies—CBT, IPSRT, and family-focused therapy—and why combining psychotherapy with medication usually works best. Practical daily strategies (sleep, routine, exercise, nutrition) and digital tools for tracking mood are highlighted as key supports. Finally, it discusses special cases like pregnancy, youth, co-occurring conditions, and how to build a safety or relapse-prevention plan with your care team.