
Introduction: When the Name Itself Is a Fear
Here is a strange fact. The official name for the fear of long words is hippopotomonstrosesquippedaliophobia. Yes, really. The word itself is long and complicated. It is almost like a joke that mental health professionals play on us. But the fear it describes is very real for many people.
If you feel anxiety when you see a word like "antidisestablishment" or "pneumonoultramicroscopicsilicovolcanoconiosis," you are not alone.

This feeling goes beyond just finding a word hard to read. For some, it triggers a deep, physical response. Your heart might race. You might feel a knot in your stomach. This is what experts call a specific phobia.
Specific phobias are more common than you might think. According to the DSM 5 criteria, a specific phobia involves a marked and persistent fear that is excessive or unreasonable, cued by a specific situation or object. For people with a fear of long words, the "object" is simply a long string of letters on a page.
This article is here to help you understand what is happening. We will look at how this type of fear connects to other conditions like acute stress disorder and crippling anxiety. We will also explore how this fits into the larger picture of specific phobias. If you have ever felt embarrassed by your reaction to a long word, keep reading. Understanding the fear is the first step to managing it. For a deeper look at how specific phobias work in general, check out our guide on specific phobias understanding the fear of long words spiders and heights.
What Is Hippopotomonstrosesquippedaliophobia? Definition and Origins
The name sounds like a joke, doesn’t it? Hippopotomonstrosesquippedaliophobia is the official term for the fear of long words. The word itself is a monster. It combines Latin and Greek roots that mean "big," "monstrous," and "long word," plus the Greek phobos for fear. Someone likely invented it as a playful jab at people who struggle with long words. But the fear it describes is no laughing matter.
In medical terms, this condition falls under the category of specific phobia. The DSM 5 criteria define a specific phobia as a marked and persistent fear that is excessive or unreasonable, triggered by a specific object or situation. For someone with this phobia, the trigger is seeing or thinking about a long or complex word (Lumen Learning).
The fear is real, even if the trigger seems unusual to others.
Clinical sources confirm that a specific phobia involves a deep, persistent anxiety that leads to avoidance behavior (Theravive). People with a fear of long words might avoid reading books, skip presentations, or even leave social situations where they might have to pronounce a big term. This avoidance can lead to crippling anxiety over time, especially if the person feels embarrassed about their fear.
The origin of the name is worth noting. It was likely made up as a self-referential joke, similar to calling a fear of long words by an extremely long name. But this does not make the condition any less valid. The DSM 5 recognizes that phobias can be triggered by almost anything, including words. Symptoms may include a racing heart, sweating, or a sense of dread, just like with any other phobia (Penn Medicine).
Understanding the name and its clinical roots can help you feel less alone. The fear is real, and it has a real place in mental health categories. If you experience this fear, you are not being silly. Your brain is reacting to a perceived threat, and that reaction is backed by the same diagnostic criteria used for fears of heights, spiders, or blood. For more on how these fears show up in daily life, you can read about anxiety attack symptoms and learn to recognize the physical signs.
How Common Are Specific Phobias? Prevalence and Demographics
So the fear of long words might sound like a rare oddity. But here’s the thing: specific phobias as a group are anything but rare. In fact, they are one of the most common mental health conditions in the United States.
Lifetime prevalence is about 12.5%. That means roughly one in eight people will experience a specific phobia at some point in their lives (Lumen Learning). To put it in real numbers, that’s over 40 million Americans. And that’s just the people who meet the full diagnostic criteria. Many more have milder fears that don’t get counted.
The most common subtypes include:

- Animal type (fear of spiders, snakes, dogs)
- Natural environment type (fear of heights, storms, water)
- Situational type (fear of flying, elevators, enclosed spaces)
The fear of long words doesn’t fall neatly into these categories, which is part of why it often gets dismissed. But the DSM-5 covers all specific phobias under one umbrella, regardless of how unusual the trigger might seem (Theravive).
When do phobias usually start?
Specific phobias tend to show up early in life. The median age of onset is around 7 to 11 years old. Many children develop fears naturally, but a phobia becomes a problem when it sticks around and starts interfering with daily life. For example, a child who avoids reading aloud or refuses to participate in class because they might stumble over a long word could be showing early signs of a fear of long words.
Are women more affected?
Yes, significantly. Women are roughly twice as likely to be diagnosed with a specific phobia as men. This gender gap holds true for most phobia subtypes. The reasons are not fully understood, but they likely involve a mix of biological, cultural, and social factors. Women may be more willing to report fear, or they may actually experience stronger fear responses in some cases.
The hidden cost: crippling anxiety
Many people with phobias feel embarrassed, so they never seek help. They adapt by avoiding their trigger, which works in the short term but often leads to crippling anxiety over time.

Avoidance can shrink a person’s world. Someone with a fear of long words might skip meetings, avoid reading contracts, or even leave jobs that require verbal presentations. Over years, this avoidance can feed into other issues like acute stress disorder or even agoraphobia treatment needs if the avoidance spreads to more situations.
The bottom line: you are not alone. Millions of people deal with some kind of specific phobia. The fear may feel isolating, but the numbers show it’s a shared human experience. Understanding how common phobias are can be the first step toward feeling less shame and more motivation to get help.
If you want to dive deeper into how different phobias compare, check out this guide on specific phobias: understanding the fear of long words, spiders, and heights to see how your experience fits into the bigger picture.
The Psychology Behind Phobias: Causes and Risk Factors
So why do some people develop a fear of long words while others find them just a bit annoying? The answer is as complex as the brain itself. Phobias don’t have a single cause. Instead, they usually come from a mix of learning experiences, genetic vulnerability, and the way your brain is wired.
How we learn to be afraid
There are three main ways people pick up specific phobias.
Classical conditioning is when a neutral thing becomes linked to a scary event. For example, if you stumbled over a huge word in front of your whole class and everyone laughed, your brain might now treat the sight of any long word as a danger signal. This pairing can happen in one powerful moment.
Observational learning is just as common. If you watched a parent or sibling react with panic or disgust when confronted with long written material, you might have absorbed that fear as your own.
Informational transmission means being told to be scared. Maybe a teacher warned you to avoid "impossible words," or a friend joked that saying certain terms wrong would make you look stupid. That warning sticks.
Research shows that these learning pathways play a major role in how specific phobias develop (NCBI StatPearls).
Your genes and your temperament
But learning alone doesn’t tell the whole story. Some people are simply born with a more reactive fear system. Twin studies suggest that specific phobias are moderately heritable, meaning genetics account for about 30 to 40 percent of the risk (A review and meta analysis of the heritability of specific phobia). Recent studies confirm that anxiety disorders, including phobias, have clear genetic roots (Clinical features and genetic mechanisms of anxiety, fear).
One key temperament trait is called behavioral inhibition. People with this trait tend to be shy, cautious, and easily startled in new situations as children. This pattern predicts a higher chance of developing phobias later in life. Scientists have even found specific genetic variations that make some people quicker to learn fear associations (The genetics of fear study suggests specific genetic variations).
The brain’s fear circuits
At the neurobiological level, two brain regions control how fear is learned and unlearned. The amygdala acts like a smoke alarm. It spots potential threats and triggers a fear response instantly. The prefrontal cortex is the rational part that can calm that alarm. But in people with phobias, the amygdala tends to be overactive while the prefrontal cortex has trouble shutting it down.
The lateral amygdala, in particular, learns to tell the difference between safe and scary cues (A genetic link between discriminative fear coding). When this system goes wrong, even neutral words can feel like real dangers. This helps explain why the fear of long words can feel so automatic and hard to reason with.
What this means for you
Understanding these causes can reduce shame. Your fear is not a personal weakness. It is a natural product of learning, genetics, and brain wiring. The good news is that all these pathways can be reversed. If you learned to be afraid, you can also learn to feel safe again.
If you relate to any of these risk factors and want to start feeling better, learning some coping skills for anxiety is a great next step.
Acute Stress vs. Phobic Reaction: Understanding the Difference
Let’s clear up a common mix-up. Not every strong fear response is a phobia. Sometimes it’s just acute stress. This matters because confusing the two can lead you to the wrong coping strategy.
Acute stress is a normal, short-lived reaction to an immediate threat. Imagine you’re about to give a presentation and you suddenly see a slide full of long, unfamiliar words. Your heart races, your palms sweat, and you feel a burst of panic. That’s acute stress. It kicks in fast, peaks quickly, and fades once the situation ends. It’s your body’s way of saying “pay attention, this is important.” It’s not a disorder.
A phobic reaction, on the other hand, is out of proportion to the actual danger. The fear of long words, for instance, is not just about feeling nervous during a presentation. It’s a persistent, unreasonable, and intense fear that leads to consistent avoidance. According to the DSM-5 criteria for specific phobia, the fear must be excessive, cued by the presence or anticipation of the trigger, and it must significantly interfere with daily life (Lumen Learning). People with this phobia might avoid reading altogether, skip classes where they might have to read aloud, or feel intense distress just thinking about long words.
Both acute stress and phobic reactions involve the same stress hormone surge and the same sympathetic nervous system “fight or flight” response. But here’s the key difference: acute stress is a temporary alarm that shuts off when the threat leaves. A phobia is a chronic alarm that keeps ringing even when there’s no real danger. People with specific phobias often go to great lengths to avoid the trigger, and the fear is highly distressing (Center for the Treatment and Study of Anxiety at UPenn). This avoidance can shrink your life over time.
Mislabeling your experience can be harmful. If you call everyday acute stress a “phobia,” you might feel more broken than you are. And if you downplay a real phobia as “just stress,” you might not seek the right help. The treatment for acute stress is often simple rest, relaxation, or breathing exercises. For a phobia, you usually need evidence-based therapy like exposure or cognitive behavioral therapy (Specific Phobia – StatPearls).
So how do you tell them apart? Ask yourself:
- Does the fear happen only in the moment, or does it pop up even when you just think about the trigger?
- Can you calm down quickly after the situation ends, or does the anxiety linger for hours?
- Are you actively avoiding situations because of the fear, or do you just feel uncomfortable during them?
If you’re experiencing a phobia rather than normal stress, don’t worry. These fears are treatable. Understanding the difference is the first step. For a deeper look at how specific phobias are diagnosed and treated, check out our guide on specific phobias.
Diagnosis and When to Seek Help
So you’ve noticed that your fear of long words goes beyond normal nervousness. Maybe you avoid reading menus, skip paragraphs in books, or feel your chest tighten just thinking about a long word. When does this become something you need to treat?
The official diagnosis for a specific phobia — including the fear of long words — follows strict guidelines. According to the DSM-5, the fear must be persistent, excessive, and unreasonable. It also has to last at least six months and cause significant distress or mess up your daily life (StatPearls). That’s the key: it’s not a one-time panic. It’s a pattern that sticks around.
Here’s what professionals look for:
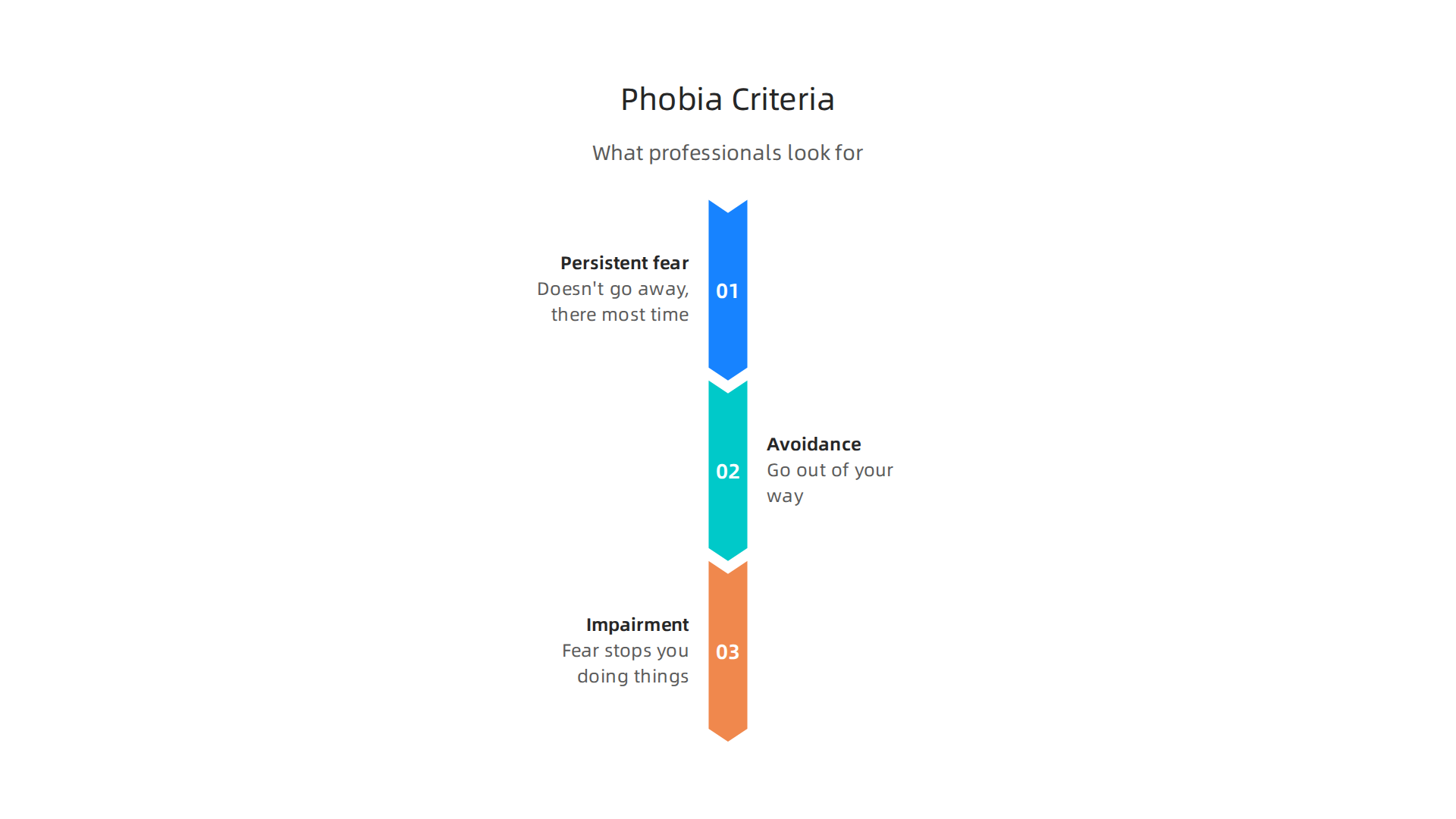
- Persistent fear. The fear of long words doesn’t go away. It’s there most of the time, not just during a stressful moment.
- Avoidance. You go out of your way to dodge situations with long words. Maybe you avoid forms, lectures, or even conversations.
- Impairment. The fear stops you from doing things you want or need to do. Your work, relationships, or school life suffers.
If you’re unsure about the severity, some self-assessment tools can help. The Social Phobia Inventory (SPIN) is one example, though it’s more for social anxiety. There are also quick online quizzes for specific phobias. But remember, these are just clues. A proper diagnosis needs a mental health professional who can rule out other conditions, like acute stress disorder or even agoraphobia treatment scenarios (Center for the Treatment and Study of Anxiety at UPenn).
When should you absolutely seek help? Look for these red flags:
- Interference with daily life. The fear of long words keeps you from reading important documents, attending work meetings, or helping your child with homework.
- Co-occurring depression or crippling anxiety. If you also feel hopeless, lose interest in activities, or have panic attacks, it’s time to call a therapist.
- Avoidance takes over. You’ve stopped going places or doing things that used to be normal for you.
Don’t wait until it gets worse. Phobias are very treatable. Exposure therapy and cognitive behavioral therapy work well (Mayo Clinic).
Start by talking to your primary care doctor or finding a licensed therapist near you.

For a more detailed breakdown of how this phobia is diagnosed and treated, check out our guide on specific phobias. You can also learn about coping skills for anxiety to manage the distress while you seek help.
The most important step is admitting that your fear is real and that you deserve relief. You don’t have to live like this. Help is available, and it starts with understanding what’s going on.
Treatment Options: Therapy, Medication, and Self-Help
Good news: your fear of long words is very treatable. In fact, specific phobias respond better to treatment than many people realize. Success rates for therapy top 70 percent for people who stick with it. That means the vast majority of people who get help see real improvement.
Let’s look at what works best.
Therapy is the Gold Standard
The most effective treatment for specific phobias is a type of therapy called cognitive-behavioral therapy (CBT). Within CBT, the key ingredient is exposure therapy. That’s where you gradually and safely face the thing you fear in small steps (StatPearls). You don’t jump into the deep end. You start with a tiny challenge, like looking at a moderately long word for a few seconds. Then you build up slowly.
According to the Mayo Clinic, exposure therapy is the best treatment for specific phobias. It works by helping your brain unlearn the fear response. Over time, your amygdala (the fear center) realizes that long words are not dangerous.
Therapists also use cognitive restructuring to change the thoughts that feed the fear. You learn to replace catastrophic thoughts with realistic ones. This combo of exposure and cognitive work is powerful.
Medication Can Help, But It’s Not the First Choice
Medication is sometimes used for phobias, but it’s usually a backup or a temporary aid. The evidence is stronger for therapy alone (Crownview Psychiatric & Wellness). Still, your doctor might suggest:
- SSRIs like sertraline or fluoxetine. These are antidepressants that can lower general anxiety. They take weeks to work.
- Beta-blockers like propranolol. These block the physical symptoms of anxiety, like a racing heart or shaky hands. They work quickly and are used for specific situations, like a work presentation.
The American Academy of Family Physicians notes that psychotherapy can be as effective as medication for anxiety disorders, and for phobias specifically, CBT has the strongest evidence (AAFP). So medication is a tool, but not the main one.
Self-Help Strategies for Mild Cases
If your fear of long words is mild and doesn’t stop you from living your life, self-help can be a great starting point.
- Gradual exposure. Make your own fear ladder. Start with a three-letter word. Then four letters. Then five. Work your way up. Do it at your own pace.
- Mindfulness and breathing. When anxiety spikes, focus on slow belly breathing. This calms your nervous system.
- Online programs. There are many evidence-based apps and courses for phobia treatment. Look for ones based on CBT principles.
Many people find that self-help alone is enough for milder fears. But if it’s not working, that’s a sign to seek professional support.
What About Severe Cases?
There are also intensive treatment programs. For example, the Bergen 4-day treatment is a condensed form of exposure therapy originally developed for OCD but now adapted for phobias (Cambridge). This shows how flexible and effective exposure-based treatments can be.
No matter where you start, the key is to begin. The fear of long words does not have to control your reading life, your work, or your confidence.
For a deeper look at how these treatments fit into a complete plan, check out our guide on specific phobias and how they are treated.
You have more options than you think. And every one of them starts with one small step.
Living with a Phobia: Coping Strategies for Daily Life
You don’t have to wait for therapy to feel better. While treatment like CBT works really well, there are things you can do right now to make daily life easier. The fear of long words can show up at work, school, or even while reading a menu. Specific phobias can affect your quality of life in many small ways, as noted by experts who study how these fears impact daily routines. Here are some practical ways to cope right now.
Acceptance and Commitment Therapy (ACT) Techniques
ACT is a different approach. Instead of fighting your fear, you learn to accept it without letting it run the show. The main goal is to reduce something called experiential avoidance. That is when you try to push away uncomfortable thoughts or feelings. The problem is, pushing them away often makes them stronger.
With ACT, you practice noticing the fear without judging it. You might say to yourself, "I notice my heart is racing because I see a long word. That is okay. I can still read this sentence anyway." This small shift can reduce crippling anxiety over time.
One simple ACT technique is called "leaves on a stream." You imagine your fearful thoughts as leaves floating down a river. You watch them come and go without grabbing onto them. This helps you see that thoughts are just thoughts, not commands you have to follow.
Support Groups and Online Communities
You are not alone in this. Many people deal with specific phobias, and connecting with them can be a huge relief. Support groups, both in person and online, give you a space to share tips and feel understood by people who get it.
Online communities are especially helpful. You can find forums or social media groups focused on anxiety and phobias. Members share what works for them, like apps that help with reading anxiety or ways to explain the phobia to coworkers. This kind of peer support reduces isolation and gives you practical ideas you might not find anywhere else. Research on coping strategies for anxiety shows that social connection is a key part of managing symptoms long term.
Workplace and School Accommodations
The fear of long words can make certain tasks feel impossible. But you have rights. In the workplace and at school, you can ask for reasonable accommodations to reduce stress.
For example, if you need to give a presentation, you could ask to avoid long words in your slides or notes. You could request extra time for reading tasks or ask for materials in a larger font to make words less overwhelming. In school, a 504 plan or an IEP can include accommodations for anxiety disorders. The key is to speak up. Many supervisors and teachers want to help, but they need to know what you are struggling with. A simple conversation can make a big difference.
These strategies will not replace professional treatment, but they can make the tough days easier. For more evidence-based techniques to handle worry and panic in the moment, check out our guide on coping skills for anxiety.
You have more control than you think. Small steps every day add up to real change.
Summary
This article explains hippopotomonstrosesquippedaliophobia—the fear of long words—and places it within the DSM-5 category of specific phobias so readers understand why an odd trigger can be a real disorder. It reviews typical symptoms (racing heart, sweating, avoidance), prevalence and demographics, and how phobias commonly begin through conditioning, observation, or being told to fear something, plus genetic and brain-circuit contributors. The piece clarifies the difference between short-lived acute stress and a persistent phobic reaction, outlines diagnostic thresholds (duration, avoidance, impairment), and summarizes effective treatments, with CBT and exposure therapy as first-line options and medication as an adjunct. Practical self-help and coping strategies—ACT techniques, breathing, gradual exposure ladders, support groups, and workplace or school accommodations—are offered so readers can start managing symptoms immediately. Overall, the article shows when to seek professional care, what therapy looks like, and simple steps to reduce daily interference from a fear of long words.